You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
About the Authors
Maria L. Geisinger, DDS, MS
Professor
University of Alabama at Birmingham
Department of Periodontology
Birmingham, AL
Janie Lee Boyesen, DDS, DMSc
Private Practice Limited to Periodontics and Implant Dentistry
Littleton, CO
Introduction
Marijuana-also called cannabis-prepared from the dried flowering tops and leaves of the female plant of Cannabis sativa, is the most widely used illicit drug in the United States. It is estimated that 52.5 million individuals in the United States used cannabis in 2021.1 Further, while cannabis remains illegal on a federal level, emerging state legislative pathways have resulted in an increase in legalization of cannabis for medicinal and recreational use; currently more than 50% of Americans reside in a state that has removed the prohibition of adult use of cannabis.2 In previous generations, the primary mode of cannabis use was smoking, but current cannabis consumption trends include an uptick in vaping and the use of cannabis-containing products, including infused foods (edibles), beverages, oils, concentrates, and topical ointments, that have become increasingly available.1 Because of the widespread prevalence of cannabis use, dental healthcare professionals are likely to encounter individuals who are regular users. In fact, a recent survey indicated that 56% of dentists reported limiting treatment in patients who were marijuana-intoxicated (or, "high").3 Additionally, 46% of surveyed dentists also reported a need to increase anesthesia when treating patients who were habitual cannabis users.3
The main psychoactive chemical of cannabis is delta-9-tetrahydrocannabinol (D9-THC).4,5 Cannabis interacts with endogenous cannabinoid receptors, CB1 and CB2. Activation of the CB1 receptors, which are located in nerve fibers found in the cerebral cortex, limbic areas, basal ganglia, cerebellum, and thalamic areas, results in the neurologic and mental health effects of cannabis.4,5 CB2 receptors are found in cells in the immune system, predominantly macrophages, and activation results in immunomodulatory effects of cannabis.4,5 In addition to D9-THC, marijuana contains other cannabinoids, including cannabidiol (CBD).6 CBD is a nonpsychotropic cannabinoid derived from cannabis and may have therapeutic value, including analgesia, muscle relaxation, anti-inflammatory and anti-allergic effects, appetite stimulation, and antiemesis.6 The US Food and Drug Administration (FDA) approved the first drug comprised of an active ingredient derived from marijuana to treat rare, severe epilepsy in June 2018, and ongoing research is investigating the therapeutic uses of other cannabis-derived compounds.7 This course reviews the active compounds present in cannabis, the pharmacology of such compounds, the current evidence regarding cannabis use, and the oral health and clinical implications of cannabis use for patients and dental healthcare professionals.
Prevalence of Cannabis Use
Cannabis is the most commonly used federally illegal drug in the United States; 52.5 million people, or about 19% of Americans, used it at least once in 2021.1,8 Reports of use have increased considerably in a pattern that aligns with nationwide legalization efforts. In the period from 2013 to 2023, individuals reporting use of marijuana rose from 7% to 17% and those reporting that they have tried marijuana at least once rose from 38% to 50%. This may represent a true increase in consumption or an increased willingness to report use due to decreased stigma around marijuana. While not all users can be classified as exhibiting disordered use, recent research estimated that approximately three in ten people who use cannabis have cannabis use disorder.9 The risk of developing cannabis use disorder has been reported to be greater for individuals who begin to use it before age 18 years.10
Nine percent of US adults report that they engage in "regular use" of cannabis, defined as at least 10 days of consumption per month.11 Regular usage differs by education, household income, and age.11 The highest rates of regular cannabis consumption are seen among those with a high school education or less (13%) and those living in households earning less than $24,000 per year (16%).11Such rates of regular cannabis use are more than three times the rates found among those with postgraduate degrees (5%) and those living in households earning $180,000 or more annually (5%).11 Additionally, adults younger than 50 years of age are twice as likely as those aged 65 years and older to be regular cannabis users.11 There are no statistically significant differences in cannabis use between racial/ethnic groups, and males are slightly more likely to be regular cannabis users than females (11% versus 8%, respectively).11 Geographic differences in regular use are also statistically significant.11 The highest rates of use (11%) in the United States are found in the Middle Atlantic (New York, Pennsylvania, and New Jersey) and East North Central (Wisconsin, Michigan, Illinois, Indiana, and Ohio) divisions.11 The lowest usage rates (7%) are reported in the East South Central (Kentucky, Tennessee, Mississippi, and Alabama) and the West North Central (North Dakota, Minnesota, South Dakota, Nebraska, Iowa, Kansas, and Missouri) divisions.11 Interestingly, state-level legalization of cannabis was not significantly associated with the percentage of regular cannabis users in the state nor with mean days per month of cannabis use.11
Methods of cannabis consumption are also changing. While smoking of inhalational cannabis continues to be the most common form of cannabis use, an increasing percentage of individuals who report using cannabis report intake via vaping and edible use. One study showed that between 2017 and 2019, the rate of vaping as the primary form of cannabis consumption increased by approximately 5%, from 9.9 % to 14.9% of users.12 Further, the popularity of edible forms of cannabis have increased considerably. National data suggest 30% of adults and 47% of 18- to 34-year-old marijuana users have consumed marijuana in edible form.13,14 Rates of edible consumption were higher in states with legalized recreational marijuana compared with those with legalization for medical use only or no legalization.14 It is important for dental healthcare professionals to understand the trends in cannabis use so that they can address the needs of their patients who may consume marijuana in various forms.
Cannabis Pharmacology
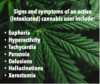
The main psychoactive chemicals in cannabis products are delta-9-tetrahydrocannabinol (D9-THC) and cannabidiol (CBD). The pharmacologic effects of each of these compounds are quite distinct. For example, CBD does not produce acute intoxication and may have anti-inflammatory, anxiolytic, and antipsychotic indications. It has also been used to treat severe refractory epilepsy in children.15 D9-THC, on the other hand, produces the acute intoxication associated with the recreational use of cannabis and has been further shown to result in undesirable effects such as paranoia, memory impairment, increased risk of psychotic illness, and cannabis dependency in some users.15 Signs of acute D9-THC intoxication are summarized in Figure 1. It should be noted that recent investigations have also highlighted the potential analgesic effect of D9-THC.15 Both D9-THC and CBD exert their effects on the body by interactions with endogenous cannabinoid receptors, CB1and CB2.16,17 In the absence of the application of exogenous cannabis, these receptors modulate neuronal activity by altering secondary neurotransmitters and the ion transport system. CB1 and CB2 receptors are both polypeptide membrane proteins that inhibit adenylate cyclase and calcium channels while they simultaneously open potassium channels.16,17 CB1 receptors are found primarily in the cerebral cortex, limbic areas, basal ganglia, cerebellum, and thalamic areas of the brain, and when acted upon by cannabis, result in activation of receptors that regulate pleasure, memory, thoughts, concentration, sensory, time perception, and coordinate voluntary movements.16,17 CB2 receptors are predominantly expressed in immune system cells, and their activation modulates cytokine release and cell migration. Cell types that express CB2 receptors include neutrophils, macrophages, B and T lymphocytes, monocytes, and mastoid cells.16,17 In many cannabis products, the ratio of D9-THC to CBD has been shown to impact the psychoactive and therapeutic potential of the cannabis product. It is thus interesting to note that the majority of both medical and recreational cannabis products (72% to 100%) in a recent market survey fall into the "most intoxicating" ratio category of THC to CBD (³ 1:1 D9-THC:CBD).15 Further, cannabis products without CBD contained the highest percentage of D9-THC (>15%).15Given the preponderance of high D9-THC content in cannabis products, consumers may be unaware of the potency of products that they are consuming.
The mode of consumption may also impact the onset and duration of symptoms. Consuming foods containing cannabis or cannabis-derived compounds; for example, D9-THC is associated with slower onset of psychoactive effects, which can be delayed by 1 to 3 hours compared with inhalational (smoking and/or vaping) methods of cannabis consumption.18 Researchers have noted that use of cannabis edibles can prolong the duration of psychoactive effects and may potentially heighten the risk of inadvertent overconsumption.19 Additionally, in 2022, the FDA issued a Consumer Alert20 that advised adults to keep cannabis edible products away from young children, due to concerns about poisoning from accidental ingestion. In fact, reported poisoning of children due to edible cannabis consumption increased 1,375% between 2017 and 2021.21
Cannabis and Oral Health
The use of cannabis, particularly marijuana smoking, has been associated with poor quality of oral health,but determination of direct causation is complicated by the number of associated factors in frequent users, including: concomitant use of tobacco, alcohol, and other drugs; poor oral hygiene practices; and infrequent visits to dentists.22-25 It has been noted that gingival conditions, including leukoplakia, leukoedema, gingival enlargement, oral dysplasia, hyperkeratosis, and even oral neoplasms are more common in individuals who use cannabis, particularly those who consume marijuana by smoking.18,25-27 Further, incidence and severity of periodontal diseases have been associated with cannabis smoking.17,28-31
Cannabis and Dental Caries
Dental caries rates, particularly smooth surface caries, have been shown to be increased in individuals who report cannabis use.18,22-25,32,33 There are potentially myriad reasons for these differences. D9-THC is an appetite stimulant and has been associated with increased carbohydrate consumption. In several studies, individuals who use cannabis report decreased frequency of toothbrushing and less regular dental visits compared with those who did not use marijuana.34 Consumption of D9-THC is also associated with an increased rate of transient xerostomia that has been shown to persist for approximately 16 hours after the use of cannabis.25Dry mouth symptoms were also noted in 69.6% of individuals after smoking cannabis compared with 18.6% of individuals after smoking tobacco.35 Further, because socioeconomic status (and therefore potentially access to dental care) has been linked to increased cannabis consumption, some studies have found that increases in caries rates in individuals who use cannabis are not statistically significant when confounders such as education level, age, and household income are considered.36,37
Cannabis Use and the Periodontium
Cannabis smoking has long been associated with increased rates of periodontitis.17,28-31 In a large longitudinal cohort study, periodontitis incidence at age 32 years among cannabis consumers was 19.3%.38 Further, individuals who had the highest levels of cannabis consumption demonstrated a significantly higher rate of development of new cases of periodontitis (RR, 1.61; 95% CI, 1.16 to 2.24)].38 It has been postulated that the deeper inhalation, prolonged oral contact with cannabis products and byproducts associated with cannabis smoking, and the absorption times of these chemicals contribute to the etiology of periodontal disease. Many of the deleterious effects of cannabis on the periodontium have been associated with the combustion products produced during cannabis smoking rather than the active ingredients in cannabis themselves.39 It should be noted that studying the effects of the combustion products can be challenging in a population cohort due to the confounding potential of concurrent tobacco consumption.40 Because much of the negative impact of cannabis use has been associated with smoking and/or vaping byproducts, it is important for the dental healthcare professional to be aware of not only cannabis consumption frequency and amount, but also mode of consumption. Currently, smoking continues to be the predominant method of cannabis consumption, with individuals who consume cannabis being three times more likely to smoke than to consume edibles.41 The main active ingredients in cannabis, cannabinoids, have been associated with the suppression of important biological pathways related to inflammation42,43 and have also been proposed as therapeutic targets for adjunctive use with periodontal therapy.16,44,45 In animal models, CBD application has been found to attenuate bone and attachment loss associated with ligature-induced periodontitis44,46 and cannabidiol essential oils have been identified as having antimicrobial properties.47-49 CBD has also been used in both animal and human models as adjuncts to improve outcomes of periodontal regeneration, including alveolar bone gain.16,50,51 Further research is necessary to better elucidate the therapeutic properties of cannabis and their utility in periodontal therapy.
Clinical Implications of Cannabis Use in Dental Patients
It has been reported that approximately 25% of dentists do not ask patients about a history of cannabis use.52 Inclusion of probative analysis of cannabis use as a part of medical and social history taking for dental patients is critically important, as such use can impact oral health, drug-drug interactions, and therapeutic outcomes for dental care. It is important for dental healthcare professionals to know if a patient uses cannabis, in what forms, and the dosages and frequency of use, as this information will allow them to better assess increased risk for oral conditions and diseases. Further, cannabinoids have been identified as inhibitors of liver enzymes, including CYP2C19 and CYP3A4/5, which can affect other medications that patients are taking that impact dental care delivery, including warfarin and clobazam.53 Cannabis has also been reported to have additional drug-drug interactions with antifungals, anti-inflammatory medications, antibiotics, analgesics, and sedative agents, impacting their clearance, potency, and duration of action.53,54 Additionally, while case reports and anecdotal evidence have suggested that individuals who regularly use cannabis may require increased dosages of a local anesthetic to achieve profound anesthesia for dental procedures,55 definitive data are not available to substantiate these claims.56
The effects of acute intoxication and their interference with delivery of dental care are also important for dental healthcare professionals to recognize. It has been recently reported that more than half of dentists surveyed reported that they have had patients arriving to appointments intoxicated with marijuana or other drugs.3 D9-THC has been shown to be associated with sinus tachycardia, atrial fibrillation, and hypertension, among other cardiovascular complications.57 Further, there is evidence to suggest that increased frequency of marijuana use increases the risk of cardiac arrhythmias and myocardial infarction in regular users.58-60 The incidence of cardiovascular complications has been estimated to be between 0.5% and 2% in individuals who were acutely intoxicated with cannabis products.61,62 Current recommendations include assessment of cannabis use prior to the delivery of dental care and avoiding elective dental care in patients for 24 hours after cannabis intoxication to reduce the risk of adverse events.63 Table 1 summarizes the recommendations for dental healthcare providers when cannabis use and/or acute intoxication is suspected in the dental office.
Therapeutic Use of Cannabis for Oral Conditions
Preliminary data suggest that the endocannabinoid system and the ways in which cannabinoids may affect periodontal tissues suggest that there may be therapeutic uses, including immunomodulatory and antimicrobial properties, that could potentially serve as adjuncts to therapies for periodontal healing and tissue regeneration.16 In animal models, cannabidiol has been shown to attenuate periodontal inflammation when applied topically.44 Further, intravenous administration of cannabidiol has been shown to mitigate bone loss in a ligature-induced periodontal inflammatory model.64 Further research focused on the potential therapeutic benefits of cannabinoid compounds for individuals with dental diseases and/or those who are undergoing dental therapies is necessary to thoroughly evaluate their potential benefits.
The Dental Professional and Cannabis
Despite the increase in number of US states that have legalized cannabis use for either medical or recreational purposes, the use of marijuana continues to be federally illegal. Use of marijuana or D9-THC-containing products by a licensed dental healthcare professional continues to be problematic. All dental boards, including those in states in which recreational marijuana use has been legalized strictly prohibit dental healthcare professionals from treating patients while abusing controlled substances, alcohol, or other chemical agents that impair the ability to practice. Further, employers have a right in all states to establish drug-free workplace policies, and most have such policies in place for safety-sensitive healthcare workplaces. Dental boards offer Diversion Programs for dentists, registered dental assistants, and dental hygienists whose marijuana or other drug use turns into a substance abuse problem. The American Dental Association (ADA) has created a Dentist Well-Being Programs Handbook for dentists dealing with personal impairment.65 Further, the ADA recommends that dental offices adopt a drug-free workplace policy to help manage office safety and offer more tools for managing drug-related issues among office staff, and provides a sample drug-free workplace policy for offices to use as a template.66
Conclusion
With the growing use of cannabis and cannabis derivatives nationwide, dental professionals may treat higher numbers of patients with a history of cannabis use and of those who may report side effects of cannabis use, including effects on the oral cavity. A thorough understanding of the impacts of cannabis on oral and overall health as well as continued assessment of current state law changes related to cannabis consumption are critical to allow the dental healthcare team to provide safe and effective treatment to all patients.
References:
1. Centers for Disease Control and Prevention. Cannabis and Public Health. About Cannabis. https://www.cdc.gov/marijuana/index.htm#:~:text=Marijuana%E2%80%94which%20can%20also%20be,people%20using%20it%20in%202019. Published February 15, 2024. Accessed September 15, 2024.
2. Carnevale Associates. Status of State Cannabis Legalization: November 2023. https://www.carnevaleassociates.com/our-work/status-of-state-cannabis-legislation-november-2023.html Accessed September 15, 2024.
3. American Dental Association. Half of Dentists Say Patients Are High at Dental Appointments. Marijuana Use May Affect Oral Health and Treatment [press release]. https://www.ada.org/en/about/press-releases/half-of-dentists-say-patients-are-high-at-dental-appointments. Published November 3, 2022. Accessed September 15, 2024.
4. Quaranta A, D'Isidoro O, Piattelli A, Hui WL, Perrotti V. Illegal drugs and periodontal conditions. Periodontol 2000. 2022;90(1):62-87.
5. Iversen L. Cannabis and the brain. Brain. 2003;126(Pt 6):1252-1270.
6. Grotenhermen F. Pharmacology of cannabinoids. Neuro Endocrinol Lett. 2004;25(1-2):14-23.
7. US Food and Drug Administration. FDA Regulation of Cannabis and Cannabis-Derived Products, Including Cannabidiol (CBD). https://www.fda.gov/news-events/public-health-focus/fda-regulation-cannabis-and-cannabis-derived-products-including-cannabidiol-cbd#:~:text=The%20FDA%20has%20approved%20Epidiolex,years%20of%20age%20and%20older. Updated July 16, 2024. Accessed September 15, 2024.
8. Substance Abuse and Mental Health Services Administration. Key substance use and mental health indicators in the United States: Results from the 2021 National Survey on Drug Use and Health (HHS Publication No. PEP22-07-01-005, NSDUH Series H-57). Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. December 2022. https://www.samhsa.gov/data/report/2021-nsduh-annual-national-report. Published December 2022. Updated April 2023. Accessed on September 15, 2024.
9. Hasin DS, Saha TD, Kerridge BT, et al. Prevalence of marijuana use disorders in the United States between 2001-2002 and 2012-2013. JAMA Psychiatry. 2015;72(12):1235-1242.
10. Winters KC, Lee C-YS. Likelihood of developing an alcohol and cannabis use disorder during youth: association with recent use and age. Drug Alcohol Depend. 2008;92(1-3):239-247.
11. Gallup News. Cannabis Use Greatest Among Lower-Income and Less Educated. https://news.gallup.com/poll/642851/cannabis-greatest-among-lower-income-less-educated.aspx#:~:text=Adults%20younger%20than%2050%2C%20for,White%2C%20Black%20and%20Hispanic%20adults. Published April 18, 2024. Accessed September 15, 2024.
12. Centers for Disease Control and Prevention. BRFSS Prevalence and Trends Data. https://www.cdc.gov/brfss/brfssprevalence/index.html. Published July 19, 2023. Accessed September 15, 2024.
13. Schauer GL, King BA, Bunnell RE, Promoff G, McAfee TA. Toking, vaping, and eating for health or fun: marijuana use patterns in adults, U.S., 2014. Am J Prev Med. 2016;50(1):1-8.
14. Steigerwald S, Wong PO, Cohen BE, et al. Smoking, vaping, and use of edibles and other forms of marijuana among U.S. adults. Ann Intern Med. 2018;169(12):890-892.
15. Pennypacker SD, Cunnane K, Cash MC, Romero-Sandoval EA. Potency and therapeutic THC and CBD ratios: US cannabis markets overshoot. Front Pharmacol. 2022;13:921493.
16. Rendón YC, Garzón HS, Bueno-Silva B, Arce RM, Suárez LJ. Cannabinoids in periodontology: where are we now? Antibiotics.2023;12(12):1687.
17. Quaranta A, D'Isidoro O, Piattelli A, Hui WL, Perrotti V. Illegal drugs and periodontal conditions. Periodontol 2000.2022;90(1):62-87.
18. Joshi S, Ashley M. Cannabis: a joint problem for patients and the dental profession. Br Dent J.2016;220(11):597-601.
19. Peralt A, Ke P, Castaneto MS. Impact of cannabis-infused edibles on public safety and regulation. J Forensic Sci. 2022;67(6):2387-2393.
20. U.S. Food and Drug Administration. FDA warns consumers about the accidental ingestion by children of food products containing THC. 2022. https://www.fda.gov/food/alerts-advisories-safety-information/fda-warns-consumers-about-accidental-ingestion-children-food-products-containing-thc. Published June 16, 2022. Accessed September 15, 2024.
21. Tweet MS, Nemanisch A, Wahl M. Pediatric Edible Cannabis Exposures and Acute Toxicity: 2017-2021. Pediatrics. 2023; 151(2):e2022057761. https://doi.org/10.1542/peds.2022-057761.
22. Schulz-Katterbach M, Imfeld T, Imfeld C. Cannabis and caries - does regular cannabis use increase the risk of caries in cigarette smokers? Schweizer Monatsschrift für Zahnmedizin SMfZ.2009;119(6):576-83.
23. Rawal SY, Tatakis DN, Tipton D. Periodontal and oral manifestations of marijuana use. J Tenn Dent Assoc. 2012;92(2):26-31.
24. Versteeg PA, Slot DE, van der Velden U, van der Weijden GA. Effect of cannabis usage on the oral environment: a review. Int J Dent Hyg. 2008;6(4):315-320.
25. Cho CM, Hirsch R, Johnstone S. General and oral health implications of cannabis use. Aust Dent J.2005;50(2):70-74.
26. Maloney WJ, Raymond GF. Common substances and medications of abuse. In: O'Neil M, ed. The ADA Practical Guide to Substance Abuse Disorders and Safe Prescribing. Hoboken, NJ: John Wiley & Sons, Inc.; 2015.
27. Alexander-Savino CV, Mirowski GW, Culton DA. Mucocutaneous manifestations of recreational drug use. Am J Clin Dermatol. 2024;25(2):281-297.
28. Darling MR. Cannabis abuse and oral health care: review and suggestions for management. SADJ. 2003;58(5):189-190.
29. Chisini LA, Cademartori MG, Francia A, et al. Is the use of cannabis associated with periodontitis? A systematic review and meta-analysis. J Periodontal Res. 2019;54(4):311-317.
30. Mayol M, Andrade E, Rivoir SP, Rossy LAB, Rösing CK. Periodontal status in cannabis smokers. A systematic review. J Int Acad Periodontol.2021;23(2):150-166.
31. Keboa MT, Enriquez N, Martel M, Nicolau B, Macdonald ME. Oral health implications of cannabis smoking: a rapid evidence review. J Can Dent Assoc. 2020;86:k2.
32. Yazdanian M, Armoon B, Noroozi A, et al. Dental caries and periodontal disease among people who use drugs: a systematic review and meta-analysis. BMC Oral Health. 2020;20(1):44.
33. Bellocchio L, Inchingolo AD, Inchingolo AM, et al. Cannabinoids drugs and oral health-from recreational side-effects to medicinal purposes: a systematic review. Int J Mol Sci. 2021;22(15):8329.
34. Schulz-Katterbach MS, Imfeld T, Imfeld C. Cannabis and caries--does regular cannabis use increase the risk of caries in cigarette smokers? Schweiz Monatsschr Zahnmed. 2009;119(6):576-583.
35. Darling MR, Arendorf TM. Effects of cannabis smoking on oral soft tissues. Community Dent Oral Epidemiol. 1993;21(2):78-81.
36. Helmi M, Aldawood A, Al-Otaibi M, Alnassar E, AlSubaie A, Aldosari M. Oral health status among recreational cannabis (marijuana and hashish) users in the USA: A NHANES-based cross-sectional study. Saudi Dent J. 2024;36(4):596-602.
37. Samman M, Scott T, Sohn W. The effect of marijuana-smoking on dental caries experience. Int Dent J. 2024;74(4):862-867.
38. Thomson WM, Poulton R, Broadbent JM, et al. Cannabis smoking and periodontal disease among young adults. JAMA.2008;299(5):525-531.
39. López R, Baelum V. Cannabis use and destructive periodontal diseases among adolescents. J Clin Periodontol. 2009;36(3):185-189.
40. Johnson GK, Slach NA. Impact of tobacco use on periodontal status. J Dent Educ. 2001;65(4):313-321.
41. Drive Research. What percentage of Americans consume edibles? https://www.driveresearch.com/percentage-americans-consume-edibles. Accessed September 15, 2024
42. Melamede R. Harm-reduction-the cannabis paradox. Harm Reduct J. 2005;2:17. doi:10.1186/1477-7517-2-17.
43. Melamed R. Cannabis and tobacco smoke are not equally carcinogenic. Harm Reduct J. 2005;2:21. doi:10.1186/1477-7517-2-21.
44. Chen H, Liu Y, Yu S, Li C, Gao B, Zhou X. Cannabidiol attenuates periodontal inflammation through inhibiting TLR4/NF-kb pathway. J Periodont Res. 2023;58(4):697-707.
45. David C, Elizalde-Hernández A, Barboza AS, Cardosa GC, Santos MBF, Moraes RR. Cannabidiol in dentistry: a scoping review. Dent J (Basel). 2022;10(10):193.
46. Gu Z, Singh S, Niyogi RG, Lamont GJ, Wang H, Lamont RJ, Scott DA. Marijuana-derived cannabinoids trigger a CB2/PI3K axis of suppression of the innate response to oral pathogens. Front Immunol. 2019;10:2288.
47. Wasim K, Haq I, Ashraf M. Antimicrobial studies of the leaf of Cannabis sativa L. Pak J Pharm Sci. 1995;8(1):29-38.
48. Nissen L, Zatta A, Stefanini I, et al. Characterization and antimicrobial activity of essential oils of industrial hemp varieties (Cannabis sativa L.) Fitoerapia. 2010;81(5):413-419.
49. van Klingeren B, ten Ham M. Antibacterial activity of D9-tetrahydrocannabinol and cannabidiol. Antonie Van Leeuwenhoek. 1976;42:9-12.
50. Napimoga MH, Benatti BB, Lima FO, Alves PM, Campos AC, Pena-Dos-Santos DR, Severina FP, Cunha FQ, Guimarães FS. Cannabidiol decreases bone resorption by inhibiting RANK/RANKL expression and pro-inflammatory cytokines during experimental periodontitis in rats. Int Immunopharmacol. 2009;9(2):216-222.
51. Hu Z, Qin Z, Xie J, Qu Y, Yin L. Cannabidiol and its application in the treatment of oral diseases: therapeutic potentials, routes of administration and prospects. Biomed Pharmacother.2024;176:116271. doi.org/10.1016/j.biopha.2024.116271.
52. Chaffee BW, Urata J, Couch ET, Silverstein S. Dental professionals' engagement in tobacco, electronic cigarette, and cannabis patient counseling. JDR Clin Trans Res.2020;5(2):133-145.
53. Antoniou T, Bodkin J, Ho JMW. Drug interactions with cannabinoids. CMAJ. 2020;192(9):E206.
54. Mittleman MA, Lewis RA, Maclure M, Sherwood JB, Muller JE. Triggering myocardial infarction by marijuana. Circulation. 2001;103(23):2805-2809.
55. Kimbrough HM Jr. Local anesthetic and the addictive patient. Tex Dent J.1975;93(5):7-9.
56. Moran MC, Heaton LJ, Leroux BG, Flake NM. Local anesthetic efficacy in marijuana users and nonusers: a pilot study. Anesth Prog. 2022;69(4):15-21.
57. Pasha AK, Clements CY, Reynolds CA, et al. Cardiovascular effects of medical marijuana: a systematic review. Am J Med.2021;134(2):182-193.
58. Hart CL, van Gorp W, Haney M, Foltin RW, Fischman MW. Effects of acute smoked marijuana on complex cognitive performance. Neuropsychopharmacology.2001;25(5):757-765.
59. Fant RV, Heishman SJ, Bunker EB, Pickworth WB. Acute and residual effects of marijuana in humans. Pharmacol Biochem Behav.1998;60(4):777-784.
60. Subramaniam VN, Menezes AR, DeSchutter A, Lavie CJ. The cardiovascular effects of marijuana: are the potential adverse effects worth the high? Mo Med. 2019;116(2):146-153.
61. Gresnigt F, van den Brink LC, Hunault C, Franssen E, de Lange D, Riezebos R. Incidence of cardiovascular symptoms and adverse events following self-reported acute cannabis intoxication at the emergency department: a retrospective study. Emerg Med J.2023;40(5):357-358.
62. Jeffers AM, Glantz S, Byers AL, Keyhani S. Association of cannabis use with cardiovascular outcomes among US adults. J Am Heart Assoc. 2024;13(5):e030178. doi.org/10.1161/JAHA.123.030178
63. American Dental Association. Cannabis: Oral Health Effects. https://www.ada.org/resources/ada-library/oral-health-topics/cannabis-oral-health-effects#:~:text=Due%20to%20concerns%20such%20as,patient98%20or%20postponing%20non%2D. Updated October 26, 2023. Accessed September 15, 2024.
64. Silveira JW, Issy AC, Castania VA, et al. Protective effects of cannabidiol on lesion-induced intervertebral disc degeneration. PLoS One. 2014;9(12):e113161.
65. American Dental Association Council on Dental Practice. Dentist Well-Being Programs Handbook. Available at: https://dentistwellbeing.com/pdf/topics_wellbeing_handbook.pdf. Accessed September 15, 2024.
66. American Dental Association Council on Dental Practice. The ADA Dentist Well-Being Programs Handbook. Appendix Drug-Free Workplace. Available at: https://toplawyer.law/wp-content/uploads/2021/10/ADA-Sample-Drug-Free-Workplace-Policy.pdf. Accessed September 15, 2024.